Jones Fractures – Greg Olsen

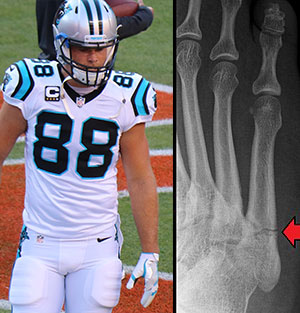
If you are a Carolina Panthers fan, as so many are in the area where we practice, you may have heard that in September, the Panthers’ Pro Bowl tight end Greg Olsen suffered an injury to his right foot. During a Sunday afternoon game, Olsen was trying to cut when he suffered a Jones fracture to his right foot. He had surgery on it the next day and has been out of the game and recovering since then. Recently, his status has changed with the team, and he is now on injured reserve (IR). He recently told the Charlotte Observer if he didn’t get back on the field this season, “I’d be very surprised.” As fans eagerly await his return, many people want to know what a Jones fracture is and why so many athletes suffer them.
Jones fractures are a common foot fracture in sports and in the community, usually with athletes (or weekend warriors) who do cutting motions. They aren’t just in football though; many other types of athletes, including several great NBA players like Shaquille O’Neal and Kevin Durant, have also suffered Jones fractures. These injuries may just be a temporary setback for many high performance athletes, but in some cases, they can eventually end careers. They can also occur from tripping or twisting the foot (even something like falling into a small hole in the yard).
So what is a Jones fracture? Why is it such a big deal?
Hopefully we can help everyone understand what it is and how it is treated.
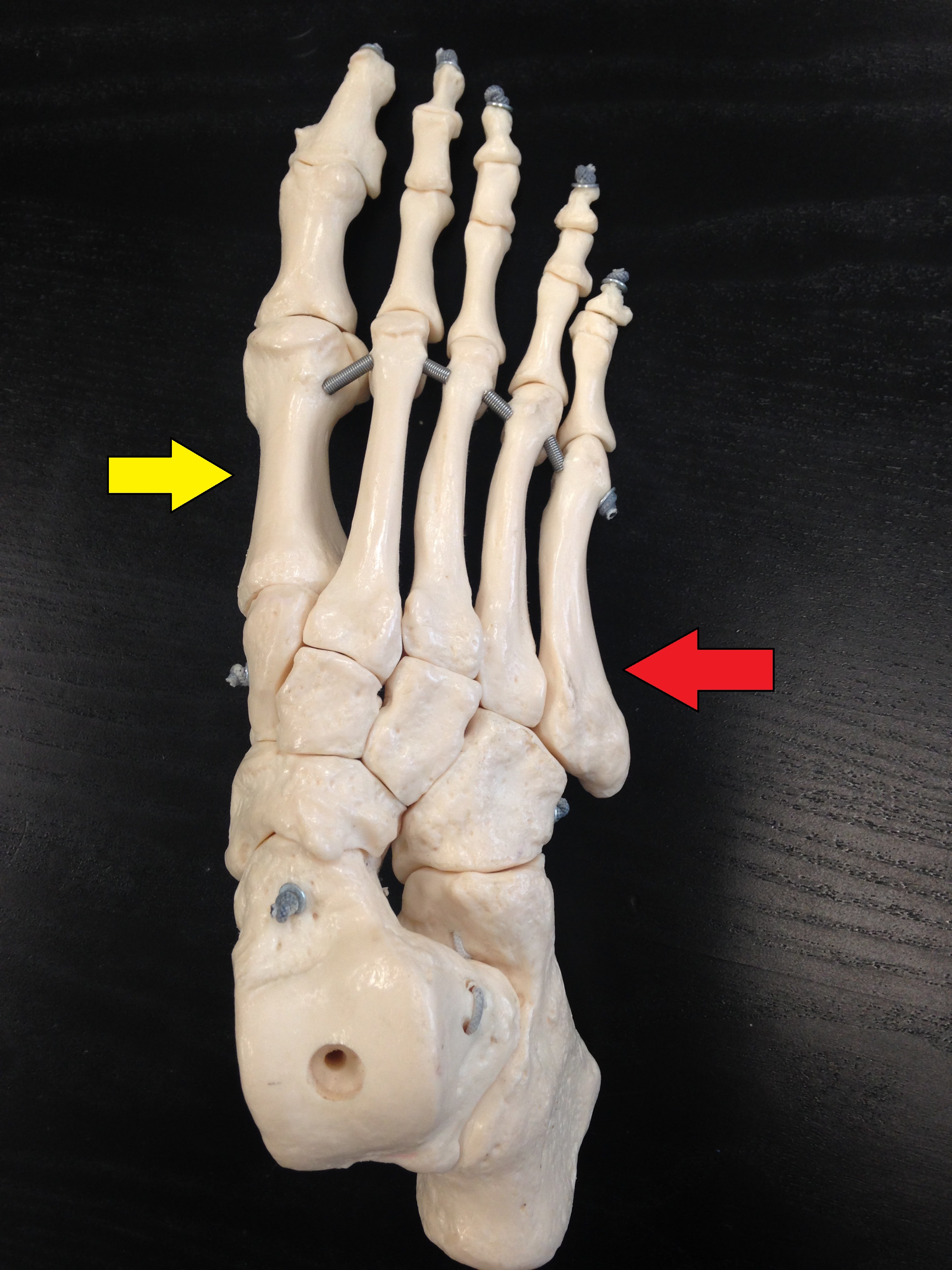
A Jones fracture is a fracture in the fifth metatarsal (a long bone on the outside middle part of the foot). You can get fractures in many different parts of that metatarsal, but the Jones is very specific. It is near the “base” of the bone (more toward the back) in an area that doesn’t have the best blood supply (red arrow).
Why is this area so important?
When healing injuries, especially bone injuries, blood flow is VERY important. The better the blood supply, the faster the healing. This fracture (break in the bone) occurs at an area that doesn’t have great blood supply and can therefore be the weakest part of the bone, making it a recipe for disaster.
Something else to consider is that, 1st metatarsal (yellow arrow) is much larger than the little 5th metatarsal (red arrow) where a Jones Fracture occurs. Our feet and knees work best when walking and running in a relatively straight line. Normally, the 1st metatarsal takes a huge amount of the load (it is bigger and stronger). But when you cut on the field or court, you have shifted most of the force onto that much smaller bone. Add in all the stuff about the blood supply, and this puts it at risk for not healing fast enough, or not at all (which we refer to as “nonunion”). But even without cutting, that bone helps to stabilize the outside of the foot with each step you take. This is why these injuries are so concerning.
What do we do about it?
In athletes, Jones fractures are usually fixed soon after the injury, in the operating room. A large screw is placed right down the middle of that bone (big screw for small bone that has poorer chance of healing), they are put in a cast for 4-6 weeks, after which they go through rehab, and are able to return to play after about 10 weeks. This is what Olsen had done, and similar treatment is often performed for many of the patients we see in our clinic.
But that isn’t the only way these injuries can be treated. Nonoperative treatment can be an option for some patients, but this requires being casted and not putting any weight on the foot for many weeks. Even then, there is a risk of not healing properly (nonunion).

Jones fractures aren’t always obvious injuries to people (unlike the “POP” and instant pain some experience with this or other fractures). Sometimes, there has been gradual onset of pain on the outside of their foot, and only after the pain becomes too much to bear or just doesn’t get any better, do patients come to see us. Sometimes, after several months, the infamous “nonunion” may already be present, meaning that the break in the bone doesn’t heal back together and you have a chronic broken bone. Yikes!

Hopefully now you have some insight into Jones fractures and why they have a reputation for being difficult to heal, even with proper and timely medical treatment. Olsen suffered a significant injury, but we will anticipate recovery and great things on the field!
If you or someone you know is experiencing an injury or pains that may indicate a Jones fracture, please contact us and schedule an appointment.
References:
Den Hartog, B D. Fracture of the Proximal Fifth Metatarsal. Journal of the American Academy of Orthopaedic Surgeons: July 2009; 17(7): 458–464.
Begly et al. Return to Play and Performance After Jones Fracture in National Basketball Association Athletes. Sports Health. 2016 Jul;8(4):342-6.
O’Malley et al. Operative Treatment of Fifth Metatarsal Jones Fractures (Zones II and III) in the NBA. Foot Ankle Int. 2016 May;37(5):488-500.
Hunt, Anderson. Treatment of Jones Fracture Nonunions and Refractures in the Elite Athlete
Outcomes of Intramedullary Screw Fixation With Bone Grafting. American Journal of Sports Medicine. 39(9): 1948-1954.
Roche, Calder. Treatment and return to sport following a Jones fracture of the fifth metatarsal: a systematic review. Knee Surgery, Sports Traumatology, Arthroscopy. June 2013; 21(6): 1307–1315.
McBryde Jr., A M. The Complicated Jones Fracture, Including Revision and Malalignment. Foot and Ankle Clinics. June 2009; 14(2): 151-168.
charlotteobserver.com/sports